
(Shutterstock)
It has been over 30 years since hip-hop superstar Tupac Shakur first told the story of 12-year-old Brenda, a sexually abused and exploited preteen mother.
I hear Brenda’s got a baby
But, Brenda’s barely got a brain
A damn shame, the girl can hardly spell her name
(That’s not our problem, that’s up to Brenda’s family)
Well let me show you how it affects our whole community
Based on real events, the lyrics shone a light on the tragic cycle of poverty, abuse, substance use and the lack of social supports for vulnerable people. They necessitate the question: How do we support children like Brenda who have been exposed to such trauma on an ongoing basis, and recognize its impact on the adults we live and work with?
As a pediatric resident physician, I regularly see patients coming from complex and exploitative social and personal situations ranging from abuse to substance use and unstable housing. These factors, which some might consider independent from treatable “medical” problems, have significant and enduring impacts on physical and mental health.
Table of Contents
Adverse childhood experiences and social determinants of health
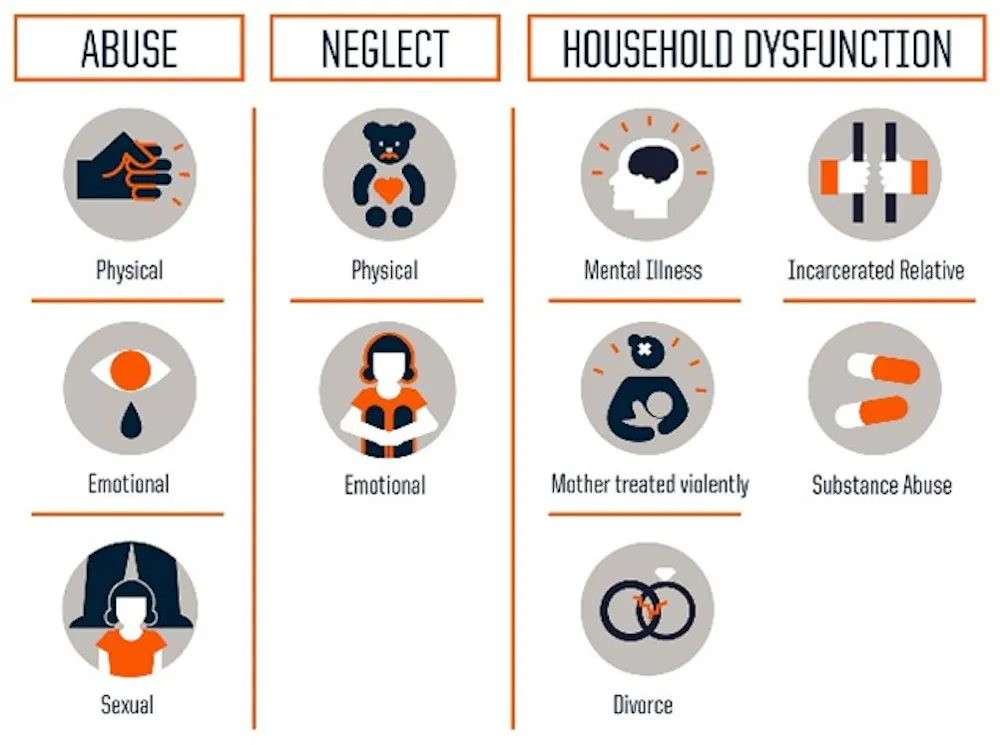
Adverse Childhood Experiences (ACEs) include:
- Emotional, physical or sexual abuse,
- Emotional or physical neglect, and
- Household challenges such as violence toward the mother, substance abuse or mental illness at home, separation or divorce, or a member of the household being incarcerated.
Exposure to ACEs, as well as disparities in social determinants of health — described by the World Health Organization as the “conditions in which people are born, grow, work, live and age” — can significantly affect development and health in children.
Exposure to ACEs is associated with physical trauma, such as traumatic brain injuries and burns; mental health issues, including depression, anxiety, suicide and PTSD; as well as other medical issues such as chronic pain, obesity and heart disease.
Beyond physical health conditions, ACEs are also associated with risky behaviours such as unsafe sex, as well as poor social outcomes such as lower education levels and income. Chronic stress can result in what is described as an allostatic load, or “wear and tear” on the body and also causes poorer health outcomes.
(Robert Wood Johnson Foundation), CC BY
The pervasiveness of exposure to these negative factors is staggering. A recent Canadian study found that over 60 per cent of adults reported experiencing at least one ACE as a child, with over one-third experiencing two or more. Poverty, a major social determinant of health, affects one in seven Canadians, and during the COVID-19 pandemic almost 15 per cent of Canadians experienced food insecurity.
Social determinants of health amount to severe disparities in health outcomes in high-income countries: for example, in Baltimore, the poorest neighbourhoods have infant mortality rates comparable to the West Bank, over ten times higher than the rates in Baltimore’s richer areas.
What can be done about ACEs and social determinants?
I regularly see the impact of ACEs and disparities in social determinants of health in my patients. I treated a young mother living in supported housing who was afraid to raise concerns about her child’s speech delay because she was worried we would call social services to apprehend her child. I met a refugee mother whose baby was admitted to hospital for poor weight gain, only for us to discover that mother was diluting her formula because she couldn’t afford more.
And I certainly remember a case similar to Brenda: a 12-year-old pregnant girl, in desperate need of both medical care and social support, who I saw in the emergency department.
Read more:
Why are babies going hungry in a food-rich nation like Canada?
As a clinician, it is frustrating that there are factors beyond our control that significantly impact patients’ health. But there are also many ways that we as clinicians and active citizens can play a role in changing these stories.

(Centers for Disease Control and Prevention), CC BY
The first is to transform how we practice medicine. As clinicians, our tool is “the social history” where we ask the questions: Who lives with you? Are there any smokers in the home? What do you do for work? and so on. But while this standard set of questions is drilled into us from medical school, their relevance can vary.
Some researchers suggest a more practical approach, focusing on domains that can be directly addressed to improve health: income, housing, education, legal status and immigration, literacy and personal safety.
Trauma-informed care
Beyond taking a better patient history, medical professionals can incorporate trauma-informed care — which recognizes the pervasiveness of trauma and responds to its effects — into our practice. We should accommodate for families in precarious social situations, whether by adapting our language to support parents with learning difficulties or by offering virtual appointment options for families with limited access to transportation.
We should recognize that intergenerational trauma and previous experiences may result in mistrust of the medical system, and focus on building bridges.
Fundamentally, we must recognize that every encounter has a social component to it — whether in a refugee health clinic or preparing for cardiac surgery, patient experiences and outcomes are influenced by social factors.
Advocating for change
As caregivers, clinicians can advocate for safe environments in homes, schools and communities. Research demonstrates that children with positive childhood experiences, such as being able to talk to family members about their feelings, feeling supported by friends or having non-parent adults take genuine interest in them, may improve adult mental health and relational health (emotional and social support networks and relationships).
Positive childhood experiences help foster resilience in children to help negate ACEs, and the strongest protective factor against ACEs is a stable relationship with an adult.
The concept of health equity focuses on allowing individuals to “reach their fullest health potential” by addressing disparities in access to care and other social determinants of health, and we should actively work to reduce these disparities. On a societal level, we can incorporate an understanding of ACEs and social determinants of health into community programming. Schools with trauma-informed practices have better results for children with exposure to ACEs.
Increased community funding for mental health supports, substance use treatment programs and universal childcare can help address household challenges. Incorporating perspectives around ACEs and social determinants of health on a community level — such as a pilot project in Tarpon Springs, Florida which incorporated a “trauma-informed lens” into policy-making — can help bring systemic change.
The impact of ACEs and social determinants of health challenges the social value placed on individuality and self-reliance. Instead, it demands societal responsibility to recognize and provide appropriate supports for children and families in precarious circumstances. We can advocate for our most vulnerable by recognizing and accommodating for these experiences. In doing so, we can all help support the Brendas in our communities.
![]()
Qaasim Mian does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.

























{kind=link}