Medically Reviewed
Dr. Jose Rossello, MD, PhD, MHCM
Preventive Medicine & Public Health Specialist
Last Reviewed: January 14, 2026
Table of Contents
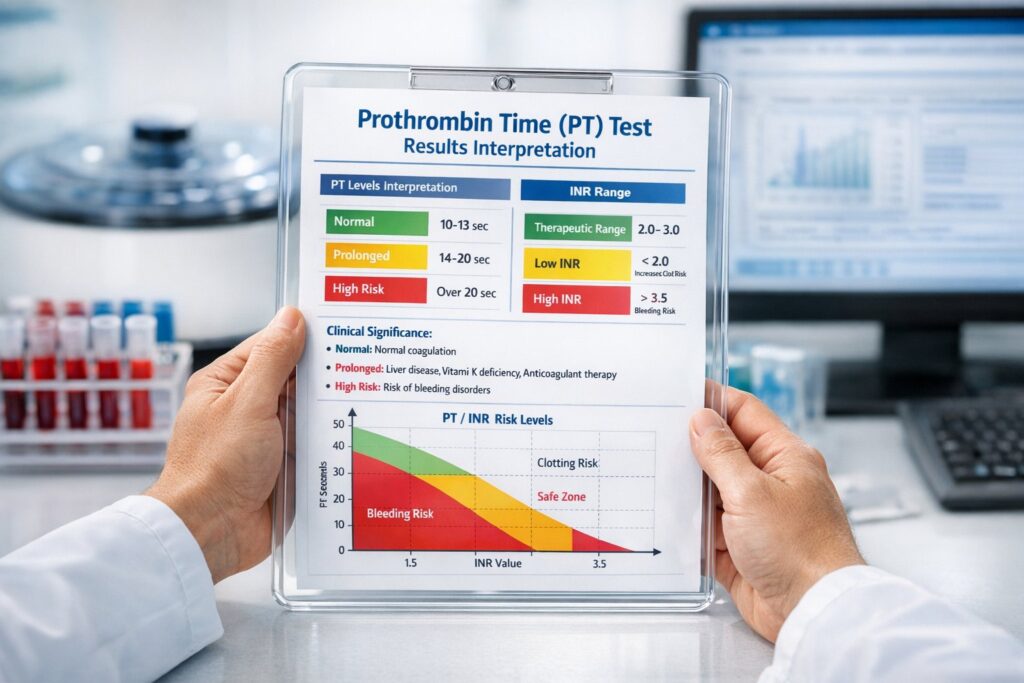
Quick Interpretation Guide
Normal Range: 10-13.5 seconds; INR of 0.8-1.1 (if not on anticoagulants)
Slightly Elevated/Low: PT 13.5-16 seconds or INR 1.1-1.5 — may indicate mild vitamin K deficiency, early liver dysfunction, or medication interaction; usually requires follow-up testing but not immediately concerning
Significantly Abnormal: PT >16 seconds or INR >3.0 — suggests substantial coagulation impairment with increased bleeding risk; requires urgent evaluation and possible intervention
Next Steps: Repeat testing if borderline, assess for liver disease and vitamin K status, review medication interactions, evaluate for bleeding disorders if prolonged without anticoagulant use
Understanding the Test
The prothrombin time (PT) is a blood coagulation test that measures how long it takes for blood plasma to clot after a standardized chemical stimulus is added. Specifically, the test evaluates the extrinsic and common pathways of the coagulation cascade, assessing the functional activity of clotting factors II (prothrombin), V, VII, and X, as well as fibrinogen levels.
The PT test answers critical clinical questions: Is your blood clotting normally? Are anticoagulant medications (like warfarin) at therapeutic levels? Do you have a bleeding disorder or liver disease affecting clotting factor production? Is your vitamin K status adequate for normal coagulation? Because different laboratories use different thromboplastin reagents that can yield varying results, the World Health Organization introduced the International Normalized Ratio (INR) as a standardized, comparable measurement across all laboratories.
The PT/INR test is most commonly ordered to monitor patients taking vitamin K antagonist anticoagulants (warfarin/Coumadin), but it’s also used when evaluating unexplained bleeding or bruising, assessing liver function, diagnosing bleeding disorders, checking coagulation status before surgery, and investigating disseminated intravascular coagulation (DIC). The test is performed by drawing a small blood sample into a special tube containing sodium citrate anticoagulant, centrifuging the sample to obtain plasma, and then adding a tissue factor reagent with calcium to initiate clotting and measure the time to clot formation.
An important limitation of the PT test is that it only evaluates the extrinsic and common pathways of coagulation—it doesn’t assess the intrinsic pathway or platelet function. Therefore, a normal PT doesn’t completely rule out all bleeding disorders. Additionally, PT results can be affected by sample collection technique (underfilled or overfilled tubes give falsely prolonged results), hematocrit levels (elevated hematocrit >55% shortens PT), lipemia, hemolysis, and the timing between sample collection and testing.
Normal Results & Reference Ranges
Standard Reference Ranges
| Patient Status | Measurement | Normal Range |
|---|---|---|
| Not on anticoagulants | PT (seconds) | 10-13.5 seconds |
| Not on anticoagulants | INR | 0.8-1.1 |
| On warfarin for atrial fibrillation/DVT/PE | INR (therapeutic) | 2.0-3.0 |
| On warfarin for mechanical heart valve | INR (therapeutic) | 2.5-3.5 |
The PT reference range varies slightly between laboratories because of differences in thromboplastin reagents, analyzers, and calibration methods. Most U.S. laboratories report a normal PT range of 10 to 13.5 seconds. The INR was standardized by the WHO to allow consistent interpretation across different laboratories using different reagents, making it the preferred method for reporting anticoagulation status.
Optimal vs Normal
A PT result within the normal range (10-13.5 seconds) indicates adequate clotting factor levels and normal coagulation in patients not taking anticoagulants. However, there’s a distinction between “normal” and “optimal” for preventive medicine purposes. Some research suggests that lower INR values (closer to 0.8-0.9) may confer optimal hemostatic balance—neither bleeding nor clotting risk. Conversely, INR values at the upper limit of normal (1.0-1.1) in patients not on anticoagulants warrant investigation, as they may herald developing liver disease, vitamin K deficiency, or early disseminated intravascular coagulation.
For patients on warfarin, the therapeutic INR target is intentionally higher (2.0-3.0 for most indications) to prevent thromboembolic events. Values consistently above 3.0 significantly increase bleeding risk without additional thromboprotection, while values below 2.0 increase clotting risk. The goal is to achieve the narrow therapeutic window that balances bleeding and clotting risks for each patient’s specific condition.
Common Causes of Abnormal Results
Most Frequent Causes of Prolonged PT/Elevated INR (Ranked by Frequency)
- Warfarin/Oral Anticoagulants (30-40% of prolonged PT) — Vitamin K antagonists intentionally prolong PT; this is the expected therapeutic effect in anticoagulated patients. However, supratherapeutic INR values (>4.0) significantly increase bleeding risk.
- Liver Disease (20-25%) — The liver synthesizes virtually all coagulation factors. Even mild hepatic dysfunction impairs production of factors II, V, VII, and X, prolonging PT. Severe liver disease shows marked PT elevation and correlates with poor prognosis.
- Vitamin K Deficiency (15-20%) — Vitamin K is essential for gamma-carboxylation of factors II, VII, IX, and X. Deficiency results from malabsorption (celiac disease, inflammatory bowel disease), antibiotic use (depleting gut flora), or inadequate dietary intake. PT elevation typically appears before other clinical signs.
- Factor Deficiency or Inhibitors (8-12%) — Inherited deficiencies of factor V, VII, X, or II cause prolonged PT. Acquired inhibitors (antiphospholipid antibodies, lupus anticoagulant) can also prolong PT despite normal factor levels.
- Disseminated Intravascular Coagulation—DIC (5-8%) — Widespread activation of coagulation consumes clotting factors and platelets system-wide, causing both prolonged PT and PTT, thrombocytopenia, and clinical bleeding. This is a medical emergency.
Most Frequent Causes of Low/Shortened PT Results (Rank by Frequency)
- Increased Vitamin K Intake or Supplementation (30-35%) — Excessive vitamin K consumption (leafy greens, supplements) antagonizes warfarin effect, lowering INR. Even dietary inconsistency causes INR instability.
- Certain Medications Inducing Warfarin Metabolism (20-25%) — Drugs that induce CYP2C9 and other hepatic enzymes increase warfarin clearance, requiring 2-5 fold dose increases. Major offenders include rifampin, carbamazepine, phenytoin, and barbiturates.
- High Hematocrit (>55%) — Polycythemia (10-15%) — Elevated red blood cell mass reduces plasma volume in the blood sample, lowering relative concentration of coagulation factors and spuriously shortening PT. Requires citrate adjustment for accurate results.
- Hypercoagulable States/Thrombophilia (8-10%) — Certain inherited thrombophilias (factor V Leiden, prothrombin G20210A mutation) and acquired hypercoagulable states show shortened PT due to elevated factor VII or fibrinogen levels.
- Acute Inflammation/Infection (5-7%) — Acute phase response elevates fibrinogen and factor VII, shortening PT. PT normalizes as inflammation resolves.
Less Common Causes
- Antiphospholipid Antibody Syndrome — Paradoxically causes prolonged PT despite hypercoagulability due to antibody interference with phospholipid-dependent coagulation tests
- Lupus Anticoagulant — Prolongs PT/aPTT in vitro but associated with thrombosis in vivo
- Severe Hyperlipidemia — Paradoxically shortens PT due to elevated fibrinogen and factor VII
- Consumptive Coagulopathies — Thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome (HUS)
- Massive Transfusion/Dilutional Coagulopathy — Dilutes clotting factors below functional threshold
- Warfarin Resistance — Rare genetic variants in VKORC1 or CYP2C9 require unusually high warfarin doses
Severity Classification
Mild Abnormality
Prolonged PT: 13.5-16 seconds; INR 1.2-1.8 (if not on warfarin)
Mild PT prolongation suggests subtle disturbance in the extrinsic or common coagulation pathways. In patients not on anticoagulants, this warrants investigation for early vitamin K deficiency, mild liver disease, or medication effects but does not immediately indicate a bleeding emergency. Clinical bleeding is uncommon with INR <1.5 in the absence of concurrent warfarin therapy. Follow-up testing in 1-2 weeks is typically recommended to determine if the abnormality is transient or persistent.
Shortened PT: <10 seconds; INR <0.7 (if not on warfarin)
Unusually short PT is uncommon and may suggest lab error, but can indicate hypercoagulability or high factor VII/fibrinogen levels. Further investigation includes repeat testing, hematocrit assessment, and evaluation for acute phase response or thrombophilia if clinically indicated.
Moderate Abnormality
Prolonged PT: 16-20 seconds; INR 1.8-3.0 (if not on warfarin, or slightly above target range if on warfarin)
Moderate PT elevation indicates substantial impairment of extrinsic/common pathway coagulation. Spontaneous bleeding risk increases significantly, particularly with mucosal surfaces (epistaxis, hematuria, melena). Further evaluation should include liver function tests, vitamin K level, medication review, mixing study (if factor inhibitor suspected), and assessment of other coagulation parameters (aPTT, platelet count, fibrinogen). If the patient is on warfarin, dose reduction is typically needed to bring INR back to target range.
Severe Abnormality
Prolonged PT: >20 seconds; INR >4.0 (in non-anticoagulated patients or significantly supratherapeutic in warfarin patients)
Severe PT prolongation represents critical impairment of coagulation and substantial bleeding risk. Spontaneous bleeding is common, including intracranial hemorrhage, gastrointestinal bleeding, and hematomas. This requires urgent evaluation and often intervention. In supratherapeutic warfarin patients, INR >4.0 warrants discussion with the anticoagulation clinic regarding reversal strategies (vitamin K, FFP, or prothrombin complex concentrate). In non-anticoagulated patients, severe PT elevation suggests critical illness—severe liver failure, massive DIC, or severe factor deficiency—requiring immediate specialist consultation and possible ICU monitoring.
Associated Symptoms & Clinical Patterns
Prolonged PT with easy bruising and petechiae often indicates vitamin K deficiency or mild bleeding disorder, especially if preceded by antibiotic use or GI symptoms.
Prolonged PT with jaundice, ascites, and encephalopathy strongly suggests advanced liver disease with synthetic dysfunction.
Prolonged PT with unexplained hemorrhage (hematemesis, melena, hematuria, intracranial bleeding) in warfarin patients indicates supratherapeutic anticoagulation requiring urgent reversal.
Shortened PT with recurrent thrombosis (DVT, PE, arterial thrombosis) despite anticoagulation suggests hereditary or acquired hypercoagulability, or poor medication adherence.
Prolonged PT with thrombosis (paradoxical bleeding with clotting) is characteristic of antiphospholipid antibody syndrome or lupus anticoagulant—these conditions cause in vitro anticoagulation but in vivo hypercoagulability.
Prolonged PT, aPTT, and thrombocytopenia with bleeding indicates DIC, a medical emergency requiring plasma exchange, platelet transfusion, and treatment of underlying trigger.
Asymptomatic isolated PT elevation (INR 1.1-1.5, no bleeding symptoms) may be incidental finding requiring follow-up but not immediate intervention, though etiologic investigation is warranted.
Recommended Diagnostic Workup
For Prolonged PT/Elevated INR (Not on Warfarin)
- Liver Function Tests — AST, ALT, alkaline phosphatase, bilirubin, albumin, INR, prothrombin time (assess for hepatic dysfunction)
- Vitamin K Level — Direct measurement or trial of vitamin K supplementation with repeat PT in 24-48 hours
- Mixing Study — Add patient plasma 1:1 with normal plasma; if PT corrects, factor deficiency likely; if PT remains prolonged, factor inhibitor suspected
- Complete Coagulation Panel — aPTT, fibrinogen, D-dimer (to assess other pathways and rule out DIC)
- Complete Blood Count — Platelet count, hematocrit, hemoglobin
- Prothrombin Complex Concentrate or Factor Assays — If mixing study suggests inhibitor, assay for antiphospholipid antibodies, lupus anticoagulant, factor V inhibitor
For Elevated INR in Warfarin Patients
- Medication History Review — Check for new medications, supplements, or dietary changes
- Liver Function Panel — Assess for concurrent liver disease
- Drug Interaction Screening — Common interactions with antibiotics, NSAIDs, statins, antiarrhythmics
- Dietary Assessment — Review vitamin K consumption consistency
- Compliance Review — Assess adherence to warfarin dosing schedule
- INR Trend Analysis — Compare to previous values to determine if chronically elevated or acutely changed
When to Order Imaging or Specialist Consultation
- Ultrasound or CT abdomen — If liver disease suspected (ascites, hepatomegaly)
- Hepatology consultation — For significant PT elevation with other signs of liver disease
- Hematology consultation — For inherited bleeding disorders, factor inhibitors, or DIC
- Anticoagulation clinic — For warfarin dosing adjustment or reversal strategies
Age & Gender Differences
Newborns and Infants: PT is normally prolonged (12-21 seconds) at birth due to immature liver synthesis of vitamin K-dependent factors. PT normalizes within 7-10 days as hepatic function matures and vitamin K is established through feeding. All newborns receive prophylactic vitamin K at birth to prevent hemorrhagic disease.
Children: By age 6 months, PT approaches adult normal range (10-13.5 seconds). PT remains consistent throughout childhood and adolescence.
Adults (20-65 years): Standard reference range 10-13.5 seconds applies uniformly to adult men and women. Gender does not significantly affect baseline PT values.
Older Adults (>65 years): No age-related change in baseline PT is expected in healthy seniors. However, older adults have higher prevalence of liver disease, medication use, vitamin K deficiency, and malabsorption disorders—all causing PT elevation. Warfarin sensitivity increases with age; older patients typically require lower doses to achieve target INR.
Pregnancy: Physiologic hypercoagulability in pregnancy typically shortens PT slightly (by 1-2 seconds) due to increased factor VII and fibrinogen. Warfarin is contraindicated in pregnancy (especially first and third trimesters) due to teratogenicity; pregnant women requiring anticoagulation use heparin instead. PT should be monitored closely in pregnant patients on anticoagulants.
Postmenopausal Women: Estrogen deficiency does not significantly alter baseline PT, but HRT may slightly increase anticoagulant effect, potentially lowering INR in warfarin-treated women starting HRT.
Medications Affecting Results
Common Medications That INCREASE PT/INR (Increase Bleeding Risk)
- Warfarin (Coumadin) — Direct PT prolongation via factor inhibition; expected therapeutic effect at INR 2-3
- Aspirin & NSAIDs — Inhibit platelet function and potentiate warfarin effect; increase bleeding risk ~2-3 fold when combined with warfarin
- Amiodarone — Complex interaction reducing warfarin metabolism; expect 25-50% warfarin dose reduction over 6-8 weeks
- Metronidazole (Flagyl) & Fluconazole — Inhibit CYP2C9, increasing warfarin levels; expect 25-50% dose reduction
- Antibiotics — Broad-spectrum antibiotics (cephalosporins, penicillins, trimethoprim-sulfamethoxazole, fluoroquinolones) deplete vitamin K-producing gut flora; effects appear 3-5 days into therapy
- Acetaminophen — High doses (>2 g/day) increase INR by ~0.7 within 3 days of initiation; recommend monitoring and dose limitation
- Certain Statins — Fluvastatin, lovastatin, rosuvastatin, simvastatin inhibit CYP2C9; pravastatin and rosuvastatin have less interaction
Common Medications That DECREASE PT/INR (Increase Clotting Risk)
- Rifampin — Potent CYP2C9 inducer; expect 2-5 fold increase in warfarin dose requirement
- Carbamazepine — Strong CYP2C9 inducer; increases warfarin metabolism significantly
- Phenytoin — Biphasic interaction: initially increases INR (protein binding displacement), then decreases after prolonged use (enzyme induction). Also requires warfarin dose increase
- Barbiturates — Induce warfarin metabolism; increase warfarin dose requirements
- Griseofulvin — Mild CYP3A4 induction; may reduce warfarin effect
- Vitamin K Supplements — Direct antagonism to warfarin effect; even small dietary increases affect INR
Medications Requiring Close INR Monitoring When Combined with Warfarin
- Venlafaxine and SSRIs — Increased bleeding risk, doubling the risk of GI bleeding
- Corticosteroids — Increase bleeding risk, possibly via GI ulceration
- Thrombolytics — Dramatically increase bleeding when combined with warfarin
- Other anticoagulants (heparin, DOACs) — Should not be used simultaneously except in specific bridging protocols
Clinical Pearl: Always review all medications, supplements, and herbal products when INR is unstable or abnormal. Changes in antibiotic use, supplements, or OTC medications can significantly alter INR within days.
Treatment & Management
When PT/INR is Mildly Elevated (INR 1.1-1.8, Not on Warfarin)
- Assess for causes — Review medications, diet, and symptoms
- Vitamin K supplementation — 1-2 mg daily (or higher if deficiency confirmed) with repeat PT in 2-4 weeks
- Address underlying cause — Stop offending medications, treat GI disease if malabsorption suspected, recommend probiotic if on antibiotics
- Repeat testing — Check PT in 4-6 weeks to confirm correction
- Consider imaging — If liver disease suspected, order liver function tests and ultrasound
When PT/INR is Moderately Elevated (INR 1.8-3.0, Not on Warfarin)
- Urgent investigation — Obtain mixing study, liver function panel, coagulation studies
- Specialist referral — Consider hematology consultation
- Vitamin K supplementation — Higher dose (5-10 mg daily), potentially IV if severe
- Assess for bleeding — Complete physical exam; check for petechiae, hematomas, evidence of bleeding
- Imaging — Ultrasound or CT imaging to assess for spontaneous hemorrhage if symptomatic
When Warfarin Patient Has Elevated INR (>3.0)
INR 3.0-4.0: Dose reduction needed but no bleeding risk increase beyond therapeutic range. Hold warfarin 1 dose; recheck INR in 3-5 days; resume at reduced dose.
INR 4.0-6.0: Dose reduction + vitamin K (2-5 mg oral) is typically recommended. Recheck INR in 3-5 days. If patient has bleeding, oral vitamin K works over 24-48 hours; for acute life-threatening bleeding, use fresh frozen plasma (FFP) or prothrombin complex concentrate (PCC) immediately.
INR >6.0 or supratherapeutic with bleeding: Immediate reversal required:
- High-dose vitamin K — 5-10 mg IV slowly (reversal takes 12-24 hours)
- Fresh Frozen Plasma (FFP) — 10-15 mL/kg provides rapid interim correction (lasts 4-6 hours)
- Prothrombin Complex Concentrate (PCC) — Preferred over FFP; provides rapid sustained reversal (factors II, VII, IX, X)
- Consider ICU admission if life-threatening bleeding
Timeline to INR Normalization
- Vitamin K supplementation — Takes 24-48 hours to begin effect (requires synthesis of new clotting factors); full correction may take 5-7 days
- Stopping warfarin — INR begins declining within 24-36 hours (factor VII with 6-hour half-life disappears first); therapeutic effect reduction takes 2-3 days; complete normalization takes 5-7 days
- Fresh frozen plasma or PCC — Effect is immediate (1-2 hours) but temporary (4-6 hours for FFP; 12-24 hours for PCC)
- Correcting vitamin K deficiency — Persistent deficiency correction requires 2-4 weeks of supplementation depending on cause
- Resolving liver disease — Depends on severity; mild reversible dysfunction may improve over weeks; cirrhosis is irreversible
Red Flags & Urgent Signs
Seek immediate medical attention if you have:
- PT/INR abnormality PLUS signs of bleeding:
- Spontaneous or unusually heavy bruising
- Epistaxis (nosebleed) lasting >10 minutes
- Hemoptysis (coughing blood)
- Hematemesis or coffee-ground emesis (vomiting blood)
- Melena or hematochezia (black or bloody stool)
- Hematuria (blood in urine)
- Vaginal bleeding outside menses or prolonged menses (>7 days)
- Intracranial hemorrhage signs: severe headache, vision changes, weakness, speech difficulty
- PT/INR abnormality PLUS thrombotic symptoms:
- Calf pain/swelling (possible DVT)
- Chest pain/shortness of breath (possible PE)
- Focal weakness/facial drooping (possible stroke)
- Supratherapeutic INR on warfarin (>4.0) with any bleeding
- Severely prolonged PT (>20 seconds) with unexplained bleeding or hemodynamic instability
- PT elevation in setting of acute illness: sepsis, trauma, massive transfusion
Key Takeaways
- PT measures coagulation via the extrinsic pathway and is reported as INR for standardization, with normal range 10-13.5 seconds (INR 0.8-1.1) in non-anticoagulated patients
- Prolonged PT most commonly indicates warfarin use (therapeutic), liver disease, or vitamin K deficiency, requiring careful investigation for the specific cause
- Medications significantly affect PT, particularly warfarin, NSAIDs, antibiotics, and amiodarone; always review medications when INR is abnormal or unstable
- Warfarin requires INR monitoring with target range 2.0-3.0 for most indications (higher for mechanical valves), and dose adjustments based on trends rather than single values
- Vitamin K supplementation effectively raises dangerously low PT but takes 24-48 hours to work, requiring urgent reversal (FFP or PCC) if severe bleeding occurs
- Liver disease causes elevated PT and correlates with prognosis; markedly elevated PT in a jaundiced patient suggests advanced cirrhosis and warrants hepatology consultation
Frequently Asked Questions
What if my result is slightly high (INR 1.1-1.5)?
A mildly elevated INR in a patient not on warfarin warrants investigation but isn’t immediately dangerous. Check whether you’ve started a new medication (especially antibiotics), increased vitamin K intake, or have recent liver issues. One mildly elevated value can be incidental or transient—repeat testing in 1-2 weeks is appropriate. If the elevation persists, vitamin K supplementation and further workup for liver disease or factor deficiency is reasonable. In contrast, if you’re on warfarin and your INR is 1.1-1.5, you’re underanticoagulated and at risk for clotting; your dose should be increased.
Should I repeat the test?
Yes, repeat testing is recommended in these scenarios:
- Borderline abnormal result (INR 1.1-1.5 or >3.5 on warfarin) — repeat in 3-7 days to determine if transient or persistent
- Warfarin adjustment — recheck 3-5 days after dose change
- Antibiotic or medication initiation — recheck 3-5 days after starting new drug known to interact
- Liver disease suspicion — repeat with liver function tests
- Never base major treatment decisions on a single PT value—always trend results
Conversely, if PT is stable in a patient on chronic warfarin with consistent INR values, testing frequency can decrease to every 4-12 weeks depending on stability and institutional guidelines.
What other tests should I get?
If PT is abnormal, request these supporting tests:
- Complete metabolic panel with liver function tests (AST, ALT, ALP, bilirubin, albumin)
- Complete blood count (platelet count, hematocrit)
- Fibrinogen level
- aPTT (activated partial thromboplastin time) to assess intrinsic pathway
- Mixing study (if factor inhibitor suspected)
- Vitamin K level or trial supplementation
- Blood cultures if infection suspected
- Antiphospholipid antibody panel if recurrent clotting suspected despite prolonged PT
Can my medication affect this result?
Absolutely. Medications are one of the most common causes of abnormal PT. Warfarin, NSAIDs, antibiotics (especially broad-spectrum), amiodarone, metronidazole, fluconazole, statins, SSRIs, and many others affect coagulation. Always bring a complete medication list—including OTC drugs, supplements, and herbal products—to your appointment. Even vitamin K supplements, cranberry extract, and fish oil can interact with warfarin. If your PT was normal before and suddenly abnormal, and you’ve started or stopped any medication within the past week, that’s likely the culprit.
What’s a normal result for my age?
Age does affect PT interpretation: Newborns have prolonged PT (12-21 seconds) normally—this corrects within 7-10 days. Children 6 months and older have normal PT values identical to adults (10-13.5 seconds). Older adults don’t have different normal ranges, but they do have higher prevalence of conditions causing PT abnormalities (liver disease, medications, vitamin K deficiency). Pregnancy causes slight PT shortening (~1-2 seconds) due to physiologic hypercoagulability. The standard reference range (10-13.5 seconds, INR 0.8-1.1) applies to all adults regardless of age, though interpretation considers age-related factors.
How long before results normalize with treatment?
Timeline depends on the treatment:
- Vitamin K supplementation — begins correcting PT within 24-36 hours but requires 3-5 days for partial correction and 5-7 days for full normalization of severely deficient patients
- Stopping warfarin — INR begins declining within 24 hours; full correction takes 5-7 days (much faster if vitamin K given concurrently)
- Fresh frozen plasma or PCC — corrects PT immediately (within 1-2 hours) but effect is temporary (4-6 hours for FFP, 12-24 hours for PCC); persistent correction requires vitamin K supplementation
- Treating liver disease — depends on underlying cause; mild reversible dysfunction may improve over weeks; cirrhosis is permanent
- Correcting vitamin K deficiency — 2-4 weeks of supplementation typically needed
- Stopping offending medications — PT normalizes over days to weeks depending on drug half-life and enzyme induction recovery
What if I’m on warfarin and missed a dose?
Generally, missing a single dose of warfarin is not dangerous. Take your next dose at the regularly scheduled time (do NOT double up). One missed dose typically doesn’t significantly lower INR. However, if you miss multiple doses in sequence, INR may drop below therapeutic range, increasing clotting risk. Check your INR within 3-5 days if you miss a dose. If you frequently forget doses, ask your pharmacist about pill organizers or phone reminders, or discuss switching to a direct oral anticoagulant (DOAC) which may be easier to remember.
Can I switch from warfarin to another anticoagulant?
Yes, but it requires careful transition. Direct oral anticoagulants (DOACs: dabigatran, rivaroxaban, apixaban, edoxaban) don’t require INR monitoring and have fewer drug interactions, but they cost more and can’t be easily reversed (except dabigatran and apixaban which have reversal agents). Your doctor should guide the transition protocol to prevent gaps in anticoagulation. Never stop warfarin abruptly and start a DOAC simultaneously without a bridging period.
What if my INR is stable but I need surgery?
If you require an elective procedure, your anticoagulation clinic should plan the transition 5-7 days before surgery. Standard protocol involves stopping warfarin 5-6 days before surgery; INR should be 4.0), it may take longer to normalize after stopping warfarin, so plan ahead. Some patients with high clotting risk may need bridge therapy (heparin) instead of simple warfarin cessation. Restart warfarin the evening of surgery or the next day, depending on bleeding risk. Coordinate with your surgeon and anticoagulation clinic well in advance.
What does a mixing study show?
A mixing study adds your plasma 1:1 to normal control plasma and repeats the PT. If PT corrects (becomes normal), you likely have a clotting factor deficiency (inherit or acquired). If PT remains prolonged, you likely have a factor inhibitor (like lupus anticoagulant or antiphospholipid antibody) or an anticoagulant present. This test helps distinguish between factor deficiency requiring supplementation and inhibitor disorders requiring different management.
How often should I get my PT checked on warfarin?
Initial warfarin therapy: Check INR 3-5 days after initiation, then every 3-5 days until stable, then weekly for 2 weeks. Stable anticoagulation: Once your INR is consistently in the therapeutic range (2.0-3.0) for 2 weeks, monitoring frequency can decrease to every 4-12 weeks depending on individual stability. After dose change: Recheck 3-5 days after any warfarin dose adjustment. With medication/illness changes: Recheck within 1 week if new medications, antibiotics, or acute illness occurs. Keep detailed INR trend records—most anticoagulation clinics track results automatically.
What if I have liver disease—does that affect interpretation?
Yes, significantly. Liver disease decreases synthesis of all vitamin K-dependent factors (II, VII, IX, X), causing markedly elevated PT. The severity of PT elevation often correlates with liver disease severity and prognosis. A significantly elevated PT in a patient with jaundice, ascites, or encephalopathy suggests advanced cirrhosis and warrants hepatology consultation. Additionally, cirrhosis patients have impaired liver ability to metabolize drugs, including warfarin, potentially requiring lower doses if anticoagulation is needed.
When to See a Doctor
Schedule an appointment with your primary care physician if you have:
- Mildly elevated PT (INR 1.1-1.5) discovered incidentally without bleeding symptoms—needs evaluation for cause
- Stable borderline PT abnormalities—need periodic monitoring and etiologic investigation
- Easy bruising or bleeding unrelated to trauma—even with normal PT, warrants complete coagulation workup
- Recent unexplained bruising with INR 1.1-1.5—investigate for emerging vitamin K deficiency or early liver disease
- Difficult-to-control INR on stable warfarin dose—suggests medication interaction or dietary inconsistency requiring investigation
Schedule urgent same-day or next-day evaluation if you have:
- Moderately elevated PT (INR 1.8-3.0 off warfarin) with any bleeding symptoms—requires prompt etiologic diagnosis and possible specialist referral
- New PT elevation with evidence of bleeding—petechiae, hematomas, GI bleeding—needs rapid assessment for bleeding disorders
- Warfarin INR 3.0-4.0 without explanation—dose adjustment may be needed
- Stable warfarin patient with sudden INR change—suggests medication interaction or compliance issue
Seek immediate emergency care (call 911) if you have:
- Severely prolonged PT (>20 seconds) with active bleeding—life-threatening
- Warfarin INR >4.0 with signs of bleeding (hemoptysis, hematemesis, hematuria, severe headache, weakness, intracranial hemorrhage signs)
- Spontaneous severe bleeding without trauma (hemoptysis, hematemesis, melena, hematuria, intracranial hemorrhage)
- Severe bruising with hemodynamic instability (dizziness, fainting, rapid heart rate)
- Bleeding into critical sites (intracranial, intra-abdominal) regardless of PT value
Post Views: 167

























{kind=link}