
THE CANADIAN PRESS/Darryl Dyck
Over 25,000 Canadians have died from opioid overdose since 2016 — with 6,306 people dying in 2020 alone.
The overdose crisis is driven by an unregulated drug supply made up mostly of fentanyl, increasingly potent fentanyl analogues such as carfentanil, and more recently, unregulated benzodiazepines. Early in the COVID-19 pandemic, fentanyl directly contributed to 89 per cent of all overdose deaths in Ontario.
The volatility and toxicity in the unregulated drug supply continues to lead to more deaths. The British Columbia coroner’s report shows that more people died in 2021 from suspected illicit toxic drugs than ever before. In 2021, there was a 26 per cent increase in overdose deaths compared to 2020.
The Public Health Agency of Canada recently estimated that without new interventions, another 8,000 overdose deaths will occur in 2022. Addressing this devastating crisis requires bold action that includes expanding current evidence-based harm reduction and treatment services, alongside new interventions to prevent overdose deaths.
Table of Contents
Safer supply
Safer supply, the practice of providing a medical prescription for pharmaceutical drugs of known quality, is one of those new interventions. In Ontario, safer supply programs are run mostly by community health centres that specialize in providing care to our most marginalized community members. These small pilot programs are a low-barrier first step alternative to the toxic drug supply.
THE CANADIAN PRESS/Darryl Dyck
There are several research studies funded across Canada to evaluate different parts of these pilot safer supply programs. We are public health researchers involved in some of these studies, and initial results are promising.
At London’s Intercommunity Health Centre, close to 250 clients are prescribed pharmaceutical opioids as a daily-dispensed prescription that they take home and use at their discretion. A recent evaluation of this program reported decreased use of fentanyl and other street-acquired drugs, reduced hospitalizations and a dramatic decrease in overdoses among clients.
Importantly, clients reported that the program was saving their life and helped them to take steps to improve their health.
Addiction treatment models
Unfortunately, there has been opposition to safer supply programs from some in the addiction treatment community. Such opposition has the potential to undermine public support for people who use drugs and the expansion of lifesaving interventions that are urgently needed.

THE CANADIAN PRESS/Darryl Dyck
Current interventions to respond to opioid use don’t work for everyone. Opioid agonist treatments (OAT) like methadone and buprenorphine, are intended to reduce cravings for opioids and manage withdrawal symptoms, but they do not produce euphoria or the high associated with other opioids.
There are issues with both access and retention in OAT. Fewer than 70 per cent of people who are diagnosed with an opioid use disorder ever start OAT. And although retention rates vary, an Ontario study found that after one year, less than half of people who do start are still using OAT. Although there isn’t a set rule for how long someone should stay on OAT, generally longer treatment is associated with better outcomes.
Despite low retention rates, addiction medicine has been reluctant to address the barriers to care that people who use drugs have been attempting to call attention to for years.
Elevate Your Health for Just $29.99/Month
Join the Precision Wellness Subscription at My Healing 365 and get discounted services, priority coaching access, virtual care, and exclusive wellness resources to support your physical, emotional, and hormonal health.
Join for $29.99/MonthPeople who use drugs have highlighted for a long time how restrictions around take-home doses reduce people’s ability to stay in methadone programs. And they are right — when restrictions on taking home doses of methadone were loosened during the COVID-19 pandemic to facilitate physical distancing, retention to methadone improved without increased negative outcomes like overdose.
Listening to drug users
To address the toxic drug poisonings that are killing Canadians at such an alarming rate, we need to start listening to people who use drugs when they tell us what’s not working with the current system.
The war on drugs has so demonized people who use drugs that they are mostly dismissed by addiction medicine experts when they have tried to say what will help their communities.

THE CANADIAN PRESS/Darryl Dyck
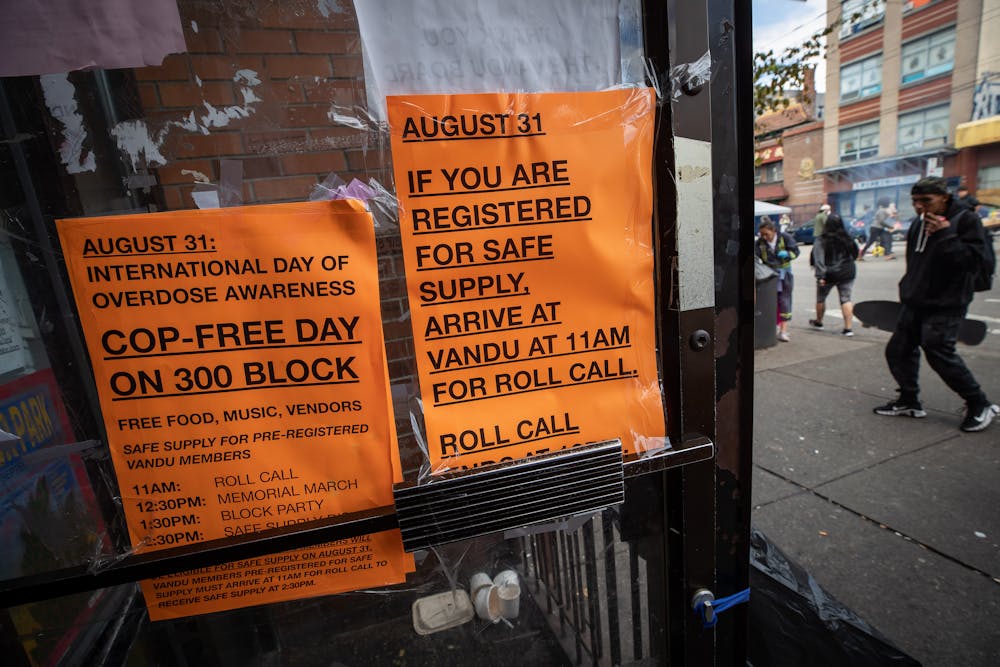
Groundbreaking grassroots work being done by organizations such as the Drug User Liberation Front (DULF) in Vancouver has highlighted the demand for a non-medicalized model for a safer supply of drugs.
DULF has organized in its community to distribute tested drugs to keep people alive during a crisis; contrast this to prominent members of the addiction medicine community attempting to use their social power to deliberately undermine their efforts.
Opposition to safer supply often misrepresents both the aim and benefits of safer supply. Safer supply is intended to keep people alive — and it works.
Building new models
We need new options. Both for people for whom current addiction treatment models have not worked and for those who simply don’t need or want treatment.
People are dying from using a toxic drug supply. Building models of care that listen to the voices of people who use drugs and centre their needs is critical and should not be dismissed based on the fears of doctors who act as gatekeepers of the status quo. The status quo did not prevent, and it will not address, the overdose crisis.
Urgent actions — like decriminalization and access to a regulated drug supply — are part of the policy changes needed to address the toxic drug crisis in Canada. But for the people at risk of drug poisoning today, and for their friends, families and loved ones, safer supply represents a real chance at preventing more tragedy.
![]()
Rose A Schmidt is employed as a research coordinator at the University of Toronto on a project that receives funding from The Ontario HIV Treatment Network about Safer Supply programs in Ontario.
Gillian Kolla receives funding from a Canadian Institutes of Health Research Banting Postdoctoral Researcher Award and a Canadian Network on Hepatitis C (CanHepC) Postdoctoral Fellowship. She has consulted for Parkdale Queen West Community Health Centre, London Intercommunity Health Centre, The Neighbourhood Group, Street Health, and The Working Centre.
Nat Kaminski is part of the University of Toronto research project on Safe Supply in Ontario, and is president of The Peel Drug Users Network & Ontario Network of People who use drugs and secretary of the Canadian Association of People who use drugs. They reviewed the guidelines for safe supply in Ontario and advocate for the expansion of services medically prescribed safe supply.

























{kind=link}